
Wayfinding in Hospitals: A Modern Approach

Most hospital leaders already know the moment. A patient arrives late, worried, and in pain. A visitor is trying to find a ward quickly. A receptionist is handling a queue while someone asks for the third set of directions in ten minutes. The building is doing important work, but the journey through it is failing people.
That is where wayfinding in hospitals stops being a signage discussion and becomes an operational one.
Hospitals are among the hardest public environments to move through effectively. Departments move. Corridors connect in ways that make sense on an estate plan but not to a first-time visitor. Clinical priorities rightly shape the building, yet the result is often a space that is hard to read, especially under stress. Good wayfinding does not remove that complexity. It helps people move through it with confidence, less interruption, and fewer avoidable delays.
The First Challenge of Healthcare Arriving
A hospital visit often becomes difficult before the clinical interaction starts.
A daughter parks, enters through the wrong entrance, follows signs for lifts, then finds that the lift lobby serves only part of the site. A patient checks a printed letter, matches the clinic name to a wall directory, walks to the right floor, then finds the department has been moved behind temporary hoarding. A volunteer points one way. A nurse, passing quickly, points another.

None of this is unusual. In fact, it is so common that many hospitals treat it as background noise. They should not.
Wayfinding is the system that helps people understand where they are, where they need to go, and how to get there. In hospitals, that system includes obvious elements such as signs, maps, colour cues, directories, landmarks, and reception desks. It also includes less visible decisions, like whether department names are consistent across appointment letters, digital screens, and room plaques.
Why arrival matters so much
The first few minutes shape the rest of the visit.
If someone arrives already flustered, every next step feels harder. Instructions are easier to miss. Time pressure feels sharper. Staff interactions start with frustration instead of focus. For patients and visitors, that feels personal. For facilities and operational leaders, it creates avoidable friction across the site.
Good wayfinding is a service layer
The best hospital wayfinding does not call attention to itself. People move.
That usually means:
- Clear decision points: Users know what to do at entrances, junctions, lifts, and department thresholds.
- Consistent naming: The place named on a letter matches the name on signs and digital systems.
- Useful final guidance: The route does not end at the right building or floor. It ends at the right door.
A hospital can offer excellent care and still create a poor experience if people cannot confidently reach it.
The Human Side of Hospital Wayfinding
The practical challenge in wayfinding in hospitals is that different users need different things from the same environment. A route that works for an employee who knows the site may fail completely for a first-time outpatient, an older visitor, or someone who is already distressed.
Patients need clarity under pressure
Patients rarely arrive in a neutral frame of mind.
Some are managing pain, fatigue, sensory overload, or anxiety about the appointment itself. Even a short route can feel hard if it involves multiple turns, lift changes, unfamiliar terminology, or conflicting signs. In that state, dense directories and long text panels are not helpful. People need simple instructions, recognisable landmarks, and reassurance that they are still on the correct path.
Hospitals also ask patients to interpret many kinds of information at once. Appointment letters, clinic names, building names, and reception instructions may all describe the same journey in slightly different language. That inconsistency creates confusion before the patient even enters the building.
Visitors make longer and more fragile journeys
Visitors often need the most complete route.
They are not just finding “Cardiology” or “Radiology”. They may need to move from car park to main entrance, from main entrance to lift bank, from lift bank to ward corridor, and from ward corridor to a specific room. If one stage fails, the whole trip stalls.
This is especially true when someone is visiting a relative in an unfamiliar part of the site. They may be emotional, in a hurry, or trying to follow verbal directions sent by text from a family member who is not sure of the route either.
A practical hospital wayfinding strategy should account for:
- Multi-stage journeys: Car park, entrance, reception, department, room.
- Different confidence levels: Frequent visitors behave differently from first-time users.
- Changing conditions: Closures, temporary routes, and relocated departments.
Staff pay the hidden operational cost
Staff are often the fallback navigation system.
That sounds manageable until you look at scale. A review focused on the UK context notes that the impact of poor hospital wayfinding on NHS staff time and productivity is significant, even though recent UK-specific quantification is limited. It also points to the scale of the NHS, with over 1.3 million staff and a 7.6 million waiting list backlog as of March 2024, making any diversion of clinical time into direction-giving an operational issue, not a minor inconvenience (analysis of wayfinding and NHS staff productivity).
That is the core problem. Every interruption seems small in isolation. Taken together, they pull attention away from patient care, front-desk flow, portering, security, and clinic operations.
When staff become the primary wayfinding tool, the hospital is using skilled people to compensate for preventable navigation failures.
Human-centred design changes the brief
The wrong brief is “How do we add more signs?”
The better brief is “How do different people successfully complete their journeys with the least confusion and least dependence on staff?” That shift changes every design choice. It moves the conversation from signage quantity to route quality, accessibility, information hierarchy, and the usefulness of digital support.
From Signs to Smartphones A Tale of Two Approaches
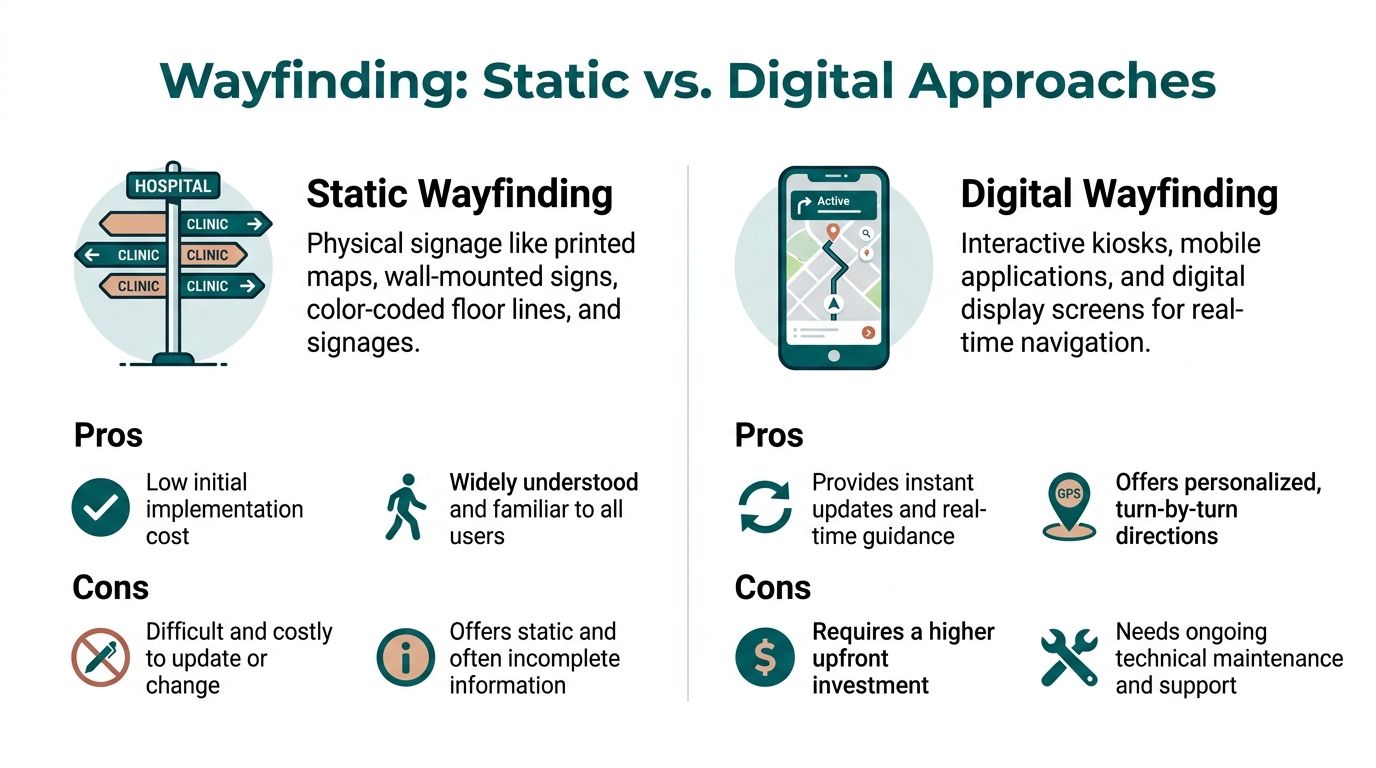
Most hospitals do not choose between static and digital wayfinding in absolute terms. They operate somewhere on a spectrum. The key decision is where each approach works, where it breaks down, and what should carry the heavier load.
What static wayfinding still does well
Traditional systems remain important.
Colour-coded zones, overhead signs, wall directories, door plaques, and floor lines help people orient themselves. They do not depend on a device, and they serve everyone in the building whether or not they planned ahead. In many hospitals, static wayfinding provides the basic structure that makes a site legible.
A long-running public hospital project reported that colour-coded, multilingual signage improved navigation success to 98%, yet many users still needed a final check with staff, particularly for harder destinations such as ICUs and operating theatres (public hospital wayfinding study).
That finding matches what many facilities teams already see on the ground. Signs can guide many individuals a significant portion of the way. The hardest part is often the last stretch, where the user must distinguish between similarly named rooms, side corridors, controlled access areas, or temporary departmental changes.
Where static systems start to fail
Hospitals are dynamic environments. Static systems are not.
A printed directory cannot react to a clinic relocation. A fixed wall sign cannot tell one user to avoid stairs and another to use the fastest route. Temporary vinyl notices can fill gaps, but too many of them make the environment harder to read, not easier.
Common weak points include:
ApproachStrengthLimitationOverhead signsGood for major destinations and route confirmationPoor at detailed final approach guidanceWall directoriesUseful for orientation near entrances and liftsQuickly outdated during moves and refurbishmentsColour zoningHelps with broad mental mappingOften too coarse for exact room-level navigationPaper mapsLow-tech fallbackHard to update and difficult under stress
What digital adds
Digital wayfinding handles change better because it can be updated without replacing physical infrastructure across the site.
That matters in hospitals, where routes shift during estates work, services move, and access conditions change. A digital system can also personalise the journey. It can guide to a named clinic, identify the correct entrance, suggest a step-free route, or support multiple languages without adding visual clutter to the walls.
This is also where the conversation about technology architecture matters. Many buyers start by looking into beacon-heavy or infrastructure-led models, then discover the maintenance burden that comes with installed hardware. Anyone reviewing options should understand the trade-offs between different indoor positioning systems, including update cycles, support requirements, and how each model behaves when the estate changes.
The practical model is digital first, not digital only
The strongest hospital environments still use signs. They just stop asking signs to do everything.
A practical operating model looks like this:
- Static signage handles orientation, reassurance, exits, and major destinations.
- Digital navigation handles precision, accessibility preferences, temporary changes, and the final approach.
- Front-line staff support exceptions rather than routine direction-giving.
Static signs are best for shared cues. Digital guidance is best for personalised journeys.
A software-first model is usually more scalable than one that depends on installed hardware throughout the estate. It is easier to update, easier to extend to new buildings, and easier to align with the pace of hospital change.
Designing for Everyone Accessibility and Compliance
Hospitals do not need wayfinding that works only for confident, sighted, tech-comfortable users. They need wayfinding that still works when a person is tired, unfamiliar with the site, moving slowly, using a wheelchair, managing low vision, or processing information differently.

That is why accessibility should not sit at the end of a procurement checklist. It should shape the whole design brief from the start.
Compliance is the floor, not the finish line
The Equality Act matters because hospitals must offer access that is practical, not symbolic.
In wayfinding terms, compliance is not just about placing some tactile elements or increasing font size on a directory. It means understanding whether a person can independently complete a journey from arrival to destination without needing special intervention every time.
That requires hospitals to look beyond the sign itself and ask harder questions:
- Visual access: Can users with low vision rely on contrast, scale, lighting, and audio alternatives?
- Physical access: Does the route guidance account for step-free travel, lift availability, and accessible entrances?
- Cognitive access: Are instructions simple, sequential, and consistent across physical and digital touchpoints?
Inclusive design usually improves the mainstream journey too
The best accessibility work often removes friction for everyone else.
Short, plain instructions help a parent carrying bags and managing a child. Step-free routing helps someone with crutches after day surgery. Clear landmarks help a visitor who does not speak English fluently. Fewer contradictory labels help everyone.
This principle shows up in adjacent design decisions as well. Even estates choices such as choosing healthcare furniture affect how legible and navigable public areas feel. Waiting zones, reception sightlines, circulation space, and clutter control all influence whether a route is easy to follow.
Build from the hardest journeys first
A reliable rule in accessibility work is to start with the most complex user need, not the average one.
If a navigation system can guide a blind or low-vision user through a hospital with confidence, many mainstream usability problems have already been addressed. Audio guidance, precise turn logic, and dependable route confirmation tend to produce a better experience for all users, not just those with access requirements. Hospitals exploring digital support for this group can review examples of products for vision impaired users as part of the requirements-setting process.
This is also where media, staff training, and public communication matter. If the system exists but no one knows how to access it, the benefit remains theoretical.
A short demonstration often helps internal stakeholders see the difference between nominal compliance and usable accessibility.
Accessibility in hospital wayfinding is not a specialist add-on. It is a core part of helping people arrive with dignity and independence.
The Roadmap to Modern Hospital Wayfinding
Hospitals often delay modern wayfinding because the project feels bigger than it is. In practice, the work becomes manageable when it is broken into phases and owned by the right people.

Start with operational alignment
The first task is not technology selection. It is agreement on the core problem.
Facilities, estates, digital, communications, outpatient operations, patient experience, accessibility leads, and front-line staff all see different parts of the issue. Bring them together early. Ask where people get lost, where staff are interrupted most often, and which journeys create the most complaints.
Useful early questions include:
- Which destinations fail most often? Entrances, clinics, imaging, wards, discharge lounges.
- Where do verbal directions repeat? Reception desks, volunteers, nurses’ stations, security points.
- What changes frequently? Temporary closures, relocations, phased refurbishments.
Build an accurate map before anything else
Digital wayfinding is only as good as its map.
That sounds obvious, but many projects underestimate the amount of detail required. A hospital map must reflect real movement, not just architectural plans. That means entrances people use, accessible routes, doors that are staff-only, lift banks that do not serve every floor, and waiting areas that act as landmarks.
A strong mapping process usually includes:
- Route validation on site by people who understand the estate in practice.
- Point-of-interest definition so that room names, clinic names, and service labels match what users see elsewhere.
- Accessibility logic that distinguishes between fastest, simplest, and step-free routes.
Test the journey, not just the software
Hospitals often approve a digital interface too early.
A map may look good on screen and still fail in the building. Testing should happen with people who represent real users, including patients, visitors, volunteers, wheelchair users, and blind or low-vision users. Observe where they hesitate, where wording is unclear, and where route instructions arrive too early or too late.
The most valuable testing question is simple. Can a first-time visitor complete the journey without asking staff?
Roll out in stages
A phased launch is usually safer than a site-wide release.
Start with one building, one service line, or one group of difficult destinations. Learn from real use. Adjust naming, route logic, communications, and staff prompts before extending across the estate.
Rollout works best when hospitals support it with visible adoption measures:
- QR codes at entrances and reception points
- Short scripts for front-desk teams
- Updated appointment messages
- Website journey pages for key clinics
This is also the stage where a hardware-free, software-first option can reduce delivery complexity. One example is Waymap, which provides indoor navigation using smartphone sensors and mapped routes rather than installed beacons or Wi-Fi dependency. In hospital settings, that model can simplify deployment where estates teams want precise guidance without adding infrastructure across multiple buildings.
Treat wayfinding as a live service
Once launched, the work is not finished.
Hospital wayfinding needs an operating model for updates. Someone must own map changes, department moves, naming consistency, and communication. That ownership matters more than the initial launch because a route that was accurate six months ago may already be wrong after estate changes.
The hospitals that get this right treat wayfinding as part of day-to-day service management, not a one-off capital project.
Measuring Success and Calculating ROI
If a hospital wants sustained investment in wayfinding, the business case has to move beyond “people like it” and into measurable operational value.
The simplest starting point is the cost of doing nothing. A landmark study by Zimring found that poor wayfinding cost a single hospital over $220,000 annually, and over 4,500 staff hours were lost each year to giving directions. Adjusted to 2025, that annual cost is over $550,000 (£440,000), with the lost hours equivalent to more than two full-time employees (breakdown of the Zimring hospital wayfinding cost study).
That figure matters because it reframes wayfinding. This is not a decorative estates issue. It is a staffing, efficiency, and service-flow issue.
What to measure in practice
Hospitals do not need a perfect analytics programme to judge whether a new approach is working. They need a sensible one.
A useful measurement set often includes:
- Direction requests: Track repeated navigation questions at reception desks, security points, and clinic check-ins.
- Late or misdirected arrivals: Review whether specific clinics report fewer patients turning up at the wrong location.
- Staff interruption patterns: Ask front-line teams whether routine direction-giving has reduced.
- Patient experience feedback: Look for comments that mention finding departments, entrances, or rooms more easily.
Separate outputs from outcomes
A hospital may launch an app, refresh signs, or install kiosks and then report activity instead of impact. Often, many projects drift here. Downloads, scans, or printed maps are outputs. They show usage. They do not show whether navigation improved.
Outcomes look different:
OutputOutcomeMore users accessed mapsFewer users asked staff for directionsMore routes were searchedMore users reached the correct department first timeMore digital content was publishedFewer temporary sign workarounds were needed
Build the ROI case around avoided friction
The strongest ROI cases usually combine three types of value.
First, there is recovered staff time. Second, there is reduced operational drag at receptions, desks, and clinic interfaces. Third, there is experience value, which is harder to price precisely but still matters because hospitals are judged on whether the visit feels organised, calm, and accessible.
A good ROI model for wayfinding does not rely on dramatic assumptions. It relies on reducing repeated, low-value friction that happens every day.
For ESG leaders, there is another layer. A modern wayfinding system can support inclusion, reduce reliance on disposable printed directions, and improve how the estate responds to changing public needs. Those are practical governance and accessibility outcomes, not branding exercises.
The Future of Navigable Healthcare Spaces
Hospitals are becoming more digital, but many still ask patients and visitors to direct themselves as if it is a paper-map problem. That gap will not hold.
The future of wayfinding in hospitals is not about replacing every sign with a screen. It is about building a navigation layer that works across the full journey, from pre-arrival information to the exact clinic door, and that adapts as the estate changes.
That matters for patient flow, but it also matters for dignity. People should not have to reveal a disability, ask for repeated help, or depend on luck to move through a healthcare environment.
The most useful systems will connect navigation to actual operations. Appointment information will point people to the correct entrance. Route guidance will reflect access needs. Estates teams will update routes quickly when layouts change. Staff will spend less time redirecting and more time doing their actual jobs.
Hospitals that want a picture of that direction of travel can look at practical deployments such as Waymap at the Royal Hospital for Children & Young People.
The broader point is straightforward. Navigable healthcare spaces are not a nice extra. They are part of how a hospital delivers care well.
Frequently Asked Questions About Hospital Wayfinding
Do hospitals still need physical signs if they add digital wayfinding
Yes.
Physical signs remain essential for orientation, reassurance, exits, and major decision points. Digital wayfinding works best when it complements signage by handling precise, personalised guidance and live updates.
What usually causes the biggest failures in hospital navigation
The common pattern is not one missing sign. It is a chain of small failures.
Examples include inconsistent department names, unclear entrances, routes that change during building works, and poor guidance for the final stretch from the correct floor to the correct room.
Is digital wayfinding only useful for large hospital campuses
No.
Large multi-building sites often feel the pain first, but smaller hospitals also benefit when layouts are complex, services move often, or accessibility needs are not well served by static signage alone.
What makes implementation difficult
The hardest part is usually governance, not software.
Hospitals need agreement on naming, route ownership, update responsibility, and testing with real users. If those pieces are weak, even a good platform will underperform.
Why do hardware-free systems get attention
Because installed hardware creates another estate to maintain.
Beacon-based or infrastructure-heavy systems can work, but they also introduce batteries, replacements, calibration, and support overhead. A software-first model is often easier to scale across changing hospital environments.
How should a hospital choose between vendors
Start with operational needs, not product features.
Ask:
- Can the system support accessible routing?
- How quickly can maps be updated after a department move?
- Does it require installed hardware?
- Can first-time visitors use it easily?
- What testing has been done with disabled users?
Who should own hospital wayfinding internally
One team rarely owns all of it well.
Facilities or estates may lead the environment, but digital, patient experience, communications, and accessibility teams all need a role. The strongest model is shared ownership with a clear operational lead.
What is the best first step if the hospital is starting from scratch
Audit the journeys that fail most often.
Do not begin by counting signs. Follow real routes from car park or entrance to destination, note where people hesitate, and record where staff repeatedly intervene. That gives you the practical brief for improvement.
If your hospital, campus, or public venue is rethinking navigation, Waymap can help you assess what a modern, accessible, hardware-free approach looks like in practice. Explore how precise indoor and outdoor navigation can support independent travel, reduce operational friction, and improve the experience of arriving.